
Non-invasive stomach monitor being developed by UC San Diego
Heart and brain activity are routinely measured through the skin with adhesive electrodes. But diagnosing gastric diseases may require patients to endure a tube stuck through the nose, down the throat and into the stomach.
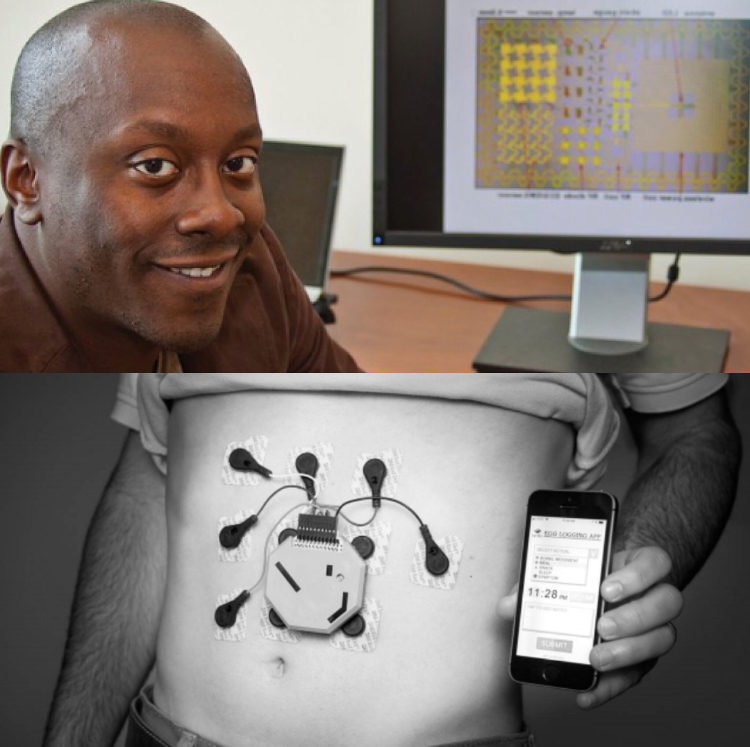
Scientists led by UC San Diego researchers say they have a better option for these patients. They’ve invented a stomach-monitoring device worn like a fanny pack.
The prototype picks up the stomach’s electrical signals through 10 electrodes stuck to the belly. Stomach activity changes with meals, sleep and other daily routines. Interruptions of these normal patterns can signal disease.
Because it can be worn for up to 24 hours, those being monitored can go about their day without being confined to a hospital or doctor’s office. It’s paired with a smartphone app, so wearers can record their activities to associate with the device’s readout.
More work is being done to refine the device to improve patient care, said Todd Coleman, a UC San Diego bioengineering professor. This perhaps could be done by licensing it for commercialization.
Children who wouldn’t tolerate getting a tube through their nose without sedation are prime subjects for this technology, Coleman said. He led the study with Armen A. Gharibans, a bioengineering postdoctoral researcher in Coleman’s lab.
The device was tested on 11 children who had simultaneously undergone monitoring via a catheter inserted through the nose, and one adult. The wearable device yielded useful and reliable data on stomach activity, the study found. Published March 22 in Nature Scientific Reports, it can be found at j.mp/stomachmonitor.
Adults can also benefit from the continuous monitoring the device provides, he said.
“A lot of these disorders are transient,” Coleman said. “Pains are not always there, and likewise for nausea.”
In addition, it may not be easy to tell if gastrointestinal problems are what they appear on the surface, or a manifestation of mental stress.
“Is this basically a brain problem manifesting in the gut? Or do you have something fundamentally wrong with your gut?” Coleman said. “We think that our technology has the potential to disambiguate that, which is huge because the treatments are very different.”
Doctors and engineers
Researchers included pediatrician Hayat Mousa of UC San Diego and Rady Children’s Hospital in San Diego; gastroenterologist David Kunkel of UCSD School of Medicine; along with UC Berkeley neurobiology scientist Benjamin Smarr. Their work is documented online at gi2.ucsd.edu.
This “marriage” of engineering and medical specialists was necessary to make a workable prototype, Coleman said. By working side by side, engineers and physicians can identify and overcome obstacles in developing solutions to medical problems, he said.
Personal motivation also made the project possible, said Coleman, whose father died of pancreatic cancer.
“It turns out he lost his mother, who passed before I was born, to stomach cancer,” Coleman said. “So it was rather personal.”
That motivation also fueled research funder Larry Smarr, a prominent UCSD physicist- futurist and father of Benjamin Smarr. The elder Smarr underwent a resection of his colon in 2016, having first assisted his surgeon by developing a high-resolution map of the region.
Coleman said he had bonded with Smarr over the years, sharing a common interest in applying data and engineering principles to medicine, and the gastrointestinal system in particular.
“When I first got to UCSD, a lot of people looked to me as a person who builds these miniaturized sensors,” Coleman said.
“Larry came to realize that my original background is really data science and data analytics. And so when he saw some of the innovative things that we were doing, he and I just realized that we’re two birds of the same feather.”
Meeting challenges
Starting around 2012, Coleman researched previous attempts to develop noninvasive gastrointestinal monitoring. Knowledge of why these attempts failed helped the team solve these pitfalls, Coleman said.
While the GI system is controlled by detectable electrical impulses, these are far fainter than the heart’s electrical signals. That makes readouts prone to interference by the body’s other electrical signals. So extracting enough usable data proved to be a challenge.
“Armen Gharibans was a new Ph.D. student in my group, and I made him aware of this ‘high-risk, high reward’ idea of trying to modernize assessment of the gut by monitoring its electrical rhythms,” Coleman said.
Coleman said he had a hunch that previous efforts had failed because there was not a close cohesion between engineers and physicians. A “seamless” team encompassing those disciplines might address the problem, he said.
“Keep in mind that at the time, this was not a sexy research area and virtually no one in the clinical community was using this readout. I applaud Armen’s willingness to nonetheless take this risk, congratulate him on his outstanding work, and am relieved that the bet paid off,” Coleman said.
bradley.fikes@sduniontribune.com